

The Ideal Aesthetic Breast

An ideally aesthetic youthful breast is positioned on the mid-portion of the chest, has a base width that extends from the sternum to the anterior axillary line, has a full rounded lower pole and a straight line sloping of the upper pole, and the nipple-areolar complex is positioned directly over the point of maximal projection (where the straight slope of the upper pole meets the rounded contour of the lower pole). This breast has healthy elastic skin, which is adherent to the underlying glandular breast tissue, and the internal supporting structures of the breast are strong and firm.
What is Breast Ptosis?
Breast ptosis describes a sagging or drooping of the breast, but can encompass several factors. Ptosis can involve the breast gland, the breast skin, and/or the nipple-areolar complex. The ideal aesthetic relationships and contours described above are altered in the drooping breast. Sun damage, pregnancy, nursing, weight fluctuations, and aging can alter the skin and the underlying supporting structures of the breast. Breast ptosis is often described in terms of the nipple position because optimal breast aesthetics depend upon the relationship of the nipple-areolar complex to the breast mound.
Glandular Ptosis
Loss of skin elasticity and stretching of the internal supporting ligaments results in drooping of the breast. As the internal structural support of the breast gland is progressively lost the breast tissue falls into the inferior portion of the skin envelope. This glandular ptosis results in the loss of upper pole fullness; and when it is more severe a concavity in the upper pole may develop. In glandular ptosis the breast (gland) volume has remained relatively stable with time, and sagging of the breast occurs primarily because of tissue stretching. The position of the nipple-areolar remains relatively stable with respect to the breast gland, and droops along with the gland as it falls inferiorly.
Breast Skin Ptosis
Breast tissue involution occurs with aging, and following breast-feeding. As the breast tissue shrinks, breast volume decreases, and the skin envelope becomes under filled. The redundant breast skin droops over the inframammary fold, and the breast usually appears wide and flat with a low nipple-areolar complex position.
Nipple-Areolar Complex Ptosis
Nipple-areolar complex ptosis describes any nipple position that is below the point of maximal breast projection; the nipple is drooping with respect to the glandular position.
Pseudoptosis
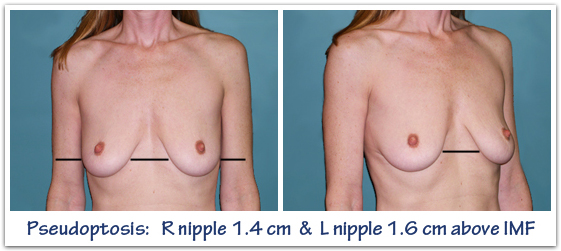
Pseudoptosis is form of glandular ptosis where the nipple remains at or above the level of the inframammary fold. When the lower pole breast skin becomes disproportionately stretched, the distance from the nipple-inframammary fold becomes disproportionately lengthened, and the breast gland falls into the lower pole. The point of maximal projection now drops below the nipple areolar complex. As pseudoptosis occurs, the nipple-areolar complex stays roughly in a stable position (but ends up in the upper breast), while the breast gland drops behind it into a stretched and enlarged inferior pole.
Classification of Breast Ptosis
To simplify, breast ptosis is often described in terms of the nipple position because optimal breast aesthetics really depends upon the relationship of the nipple-areolar complex to the breast mound and the inframammary crease. Any nipple position that is not at the point of maximal projection appears unaesthetic and detracts from the appearance of the breast. Any nipple position that is located below the level of the inframammary crease is a sure sign of breast drooping and is associated with a less than ideal breast contour. In reality, many women with ptosis have some combination of glandular, skin, and nipple-areolar complex changes that contribute to the overall drooping shape.
Breast ptosis is most commonly described by the position of the nipple in relationship to the inframammary fold.
Grade 0 – Normal – Nipple is positioned normally above the level of the inframammary crease.

Grade I – Mild – Nipple is positioned at the level of the inframammary crease; sometimes described as a nipple position 0cm – 1cm below the inframammary crease.
{insert picture}
Grade II – Moderate – Nipple is positioned below the level of the inframammary crease and above some of the lower pole breast tissue; sometimes described as a nipple position 1cm – 3cm below the inframammary crease.

Grade III – Advanced – Nipple is positioned well below the level of the inframammary crease; sometimes described as a nipple position >3cm below the inframammary crease; or the nipple points downward to the floor.

Surgical Management of Breast Ptosis
Surgical management of the NAC position is dictated by two principles: the position of the nipple in relationship to the glandular tissue, and the position of the nipple in relationship to the inframammary crease. Other related factors include tissue compliance/elasticity, skin redundancy, and the position of the breast tissue in relation to the inframammary crease. The goal is to restore a proper aesthetic relationship between the breast mound, the nipple, and the inframammary crease. There are a number of breast lift (mastopexy) techniques that can be utilized to restore breast aesthetics. If there is also a lack of breast volume then a breast implant can be used along with a breast lift.
A patient with a nipple positioned at the point of maximal projection, and that lies at the level of the inframammary crease, can be treated in several ways. Breast lift alone would certainly be one option, but most women chose breast augmentation. Filling the skin envelope by increasing breast volume may effectively raise the nipple position slightly because of tissue re-repositioning over the breast implant.
A patient with a nipple positioned at the point of maximal projection, but located below the level of the inframammary crease, will require lifting of the nipple-areolar complex as well as a reduction and tightening of the redundant skin envelope. A breast implant is used in these circumstances any time a woman desires more upper pole fullness and/or breast volume.
More to come
Trackbacks/Pingbacks